-
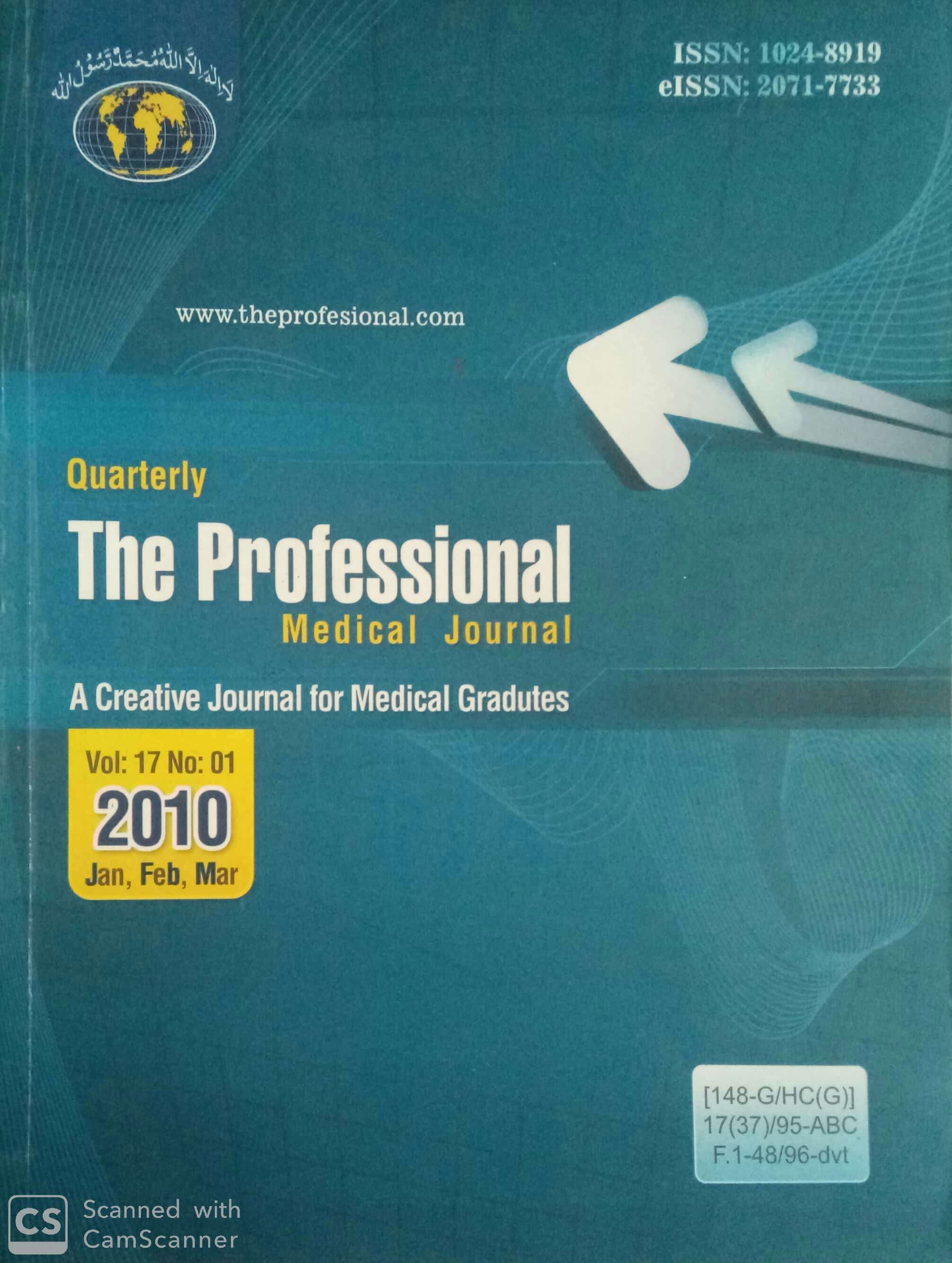
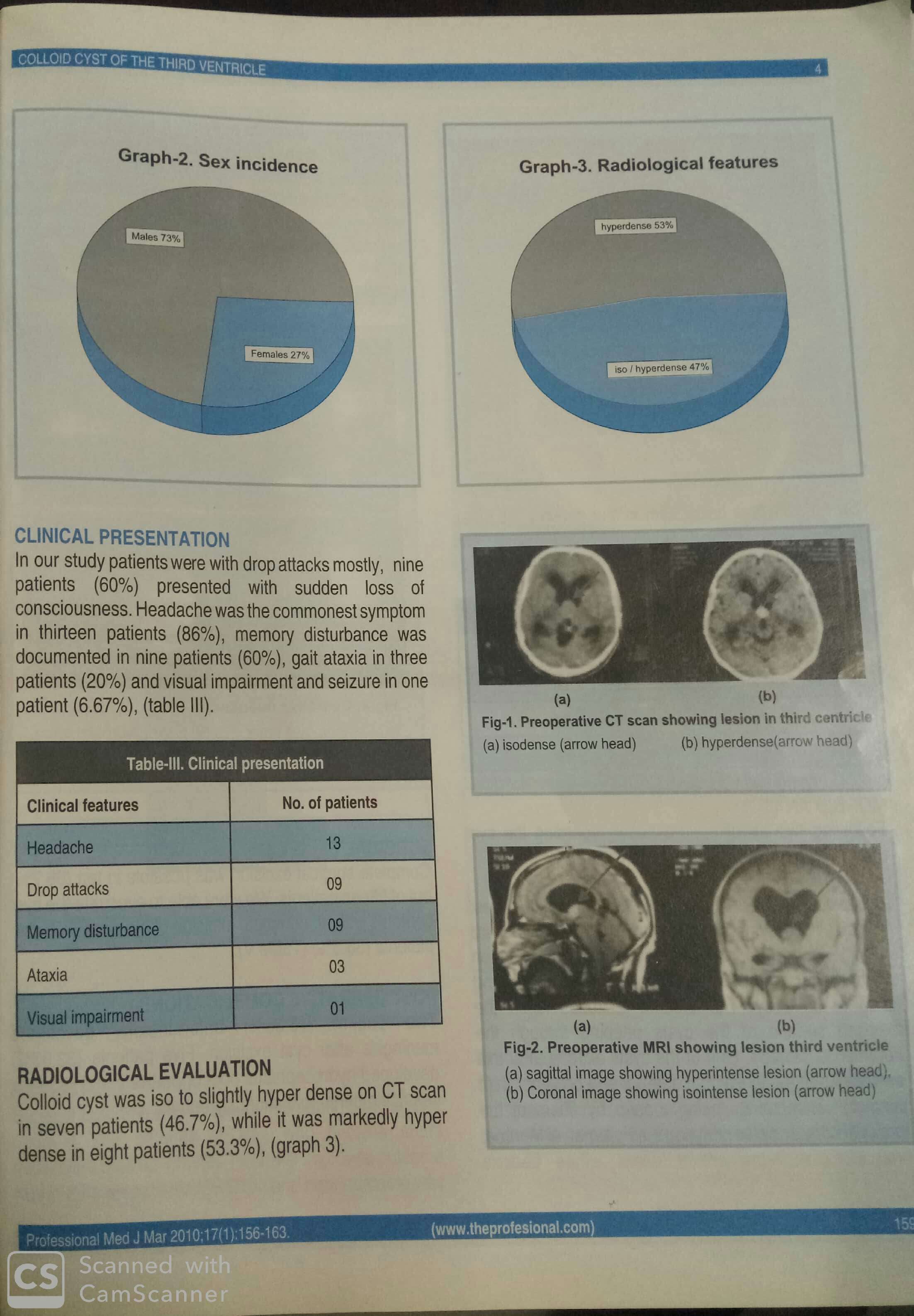
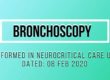
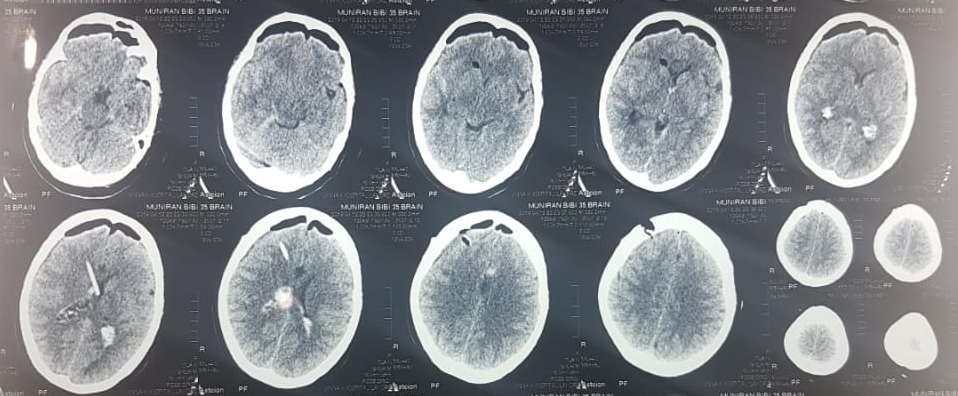
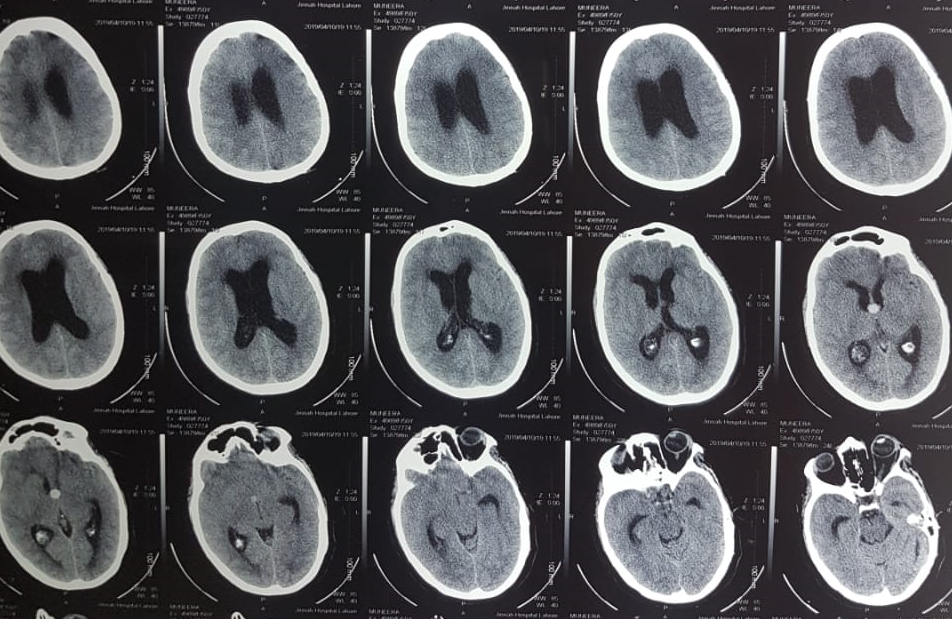
- CT Scan Brain Plain
-
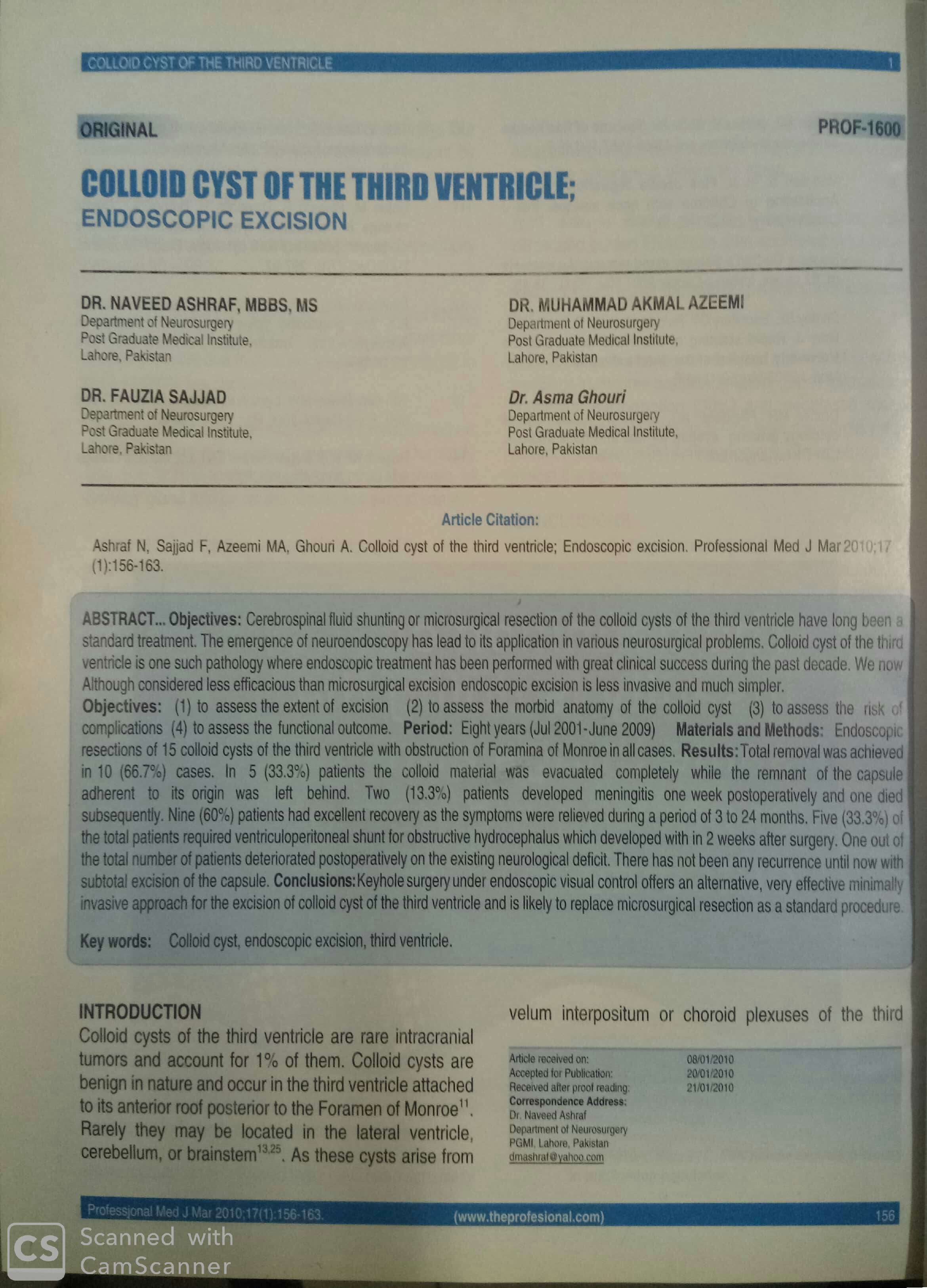
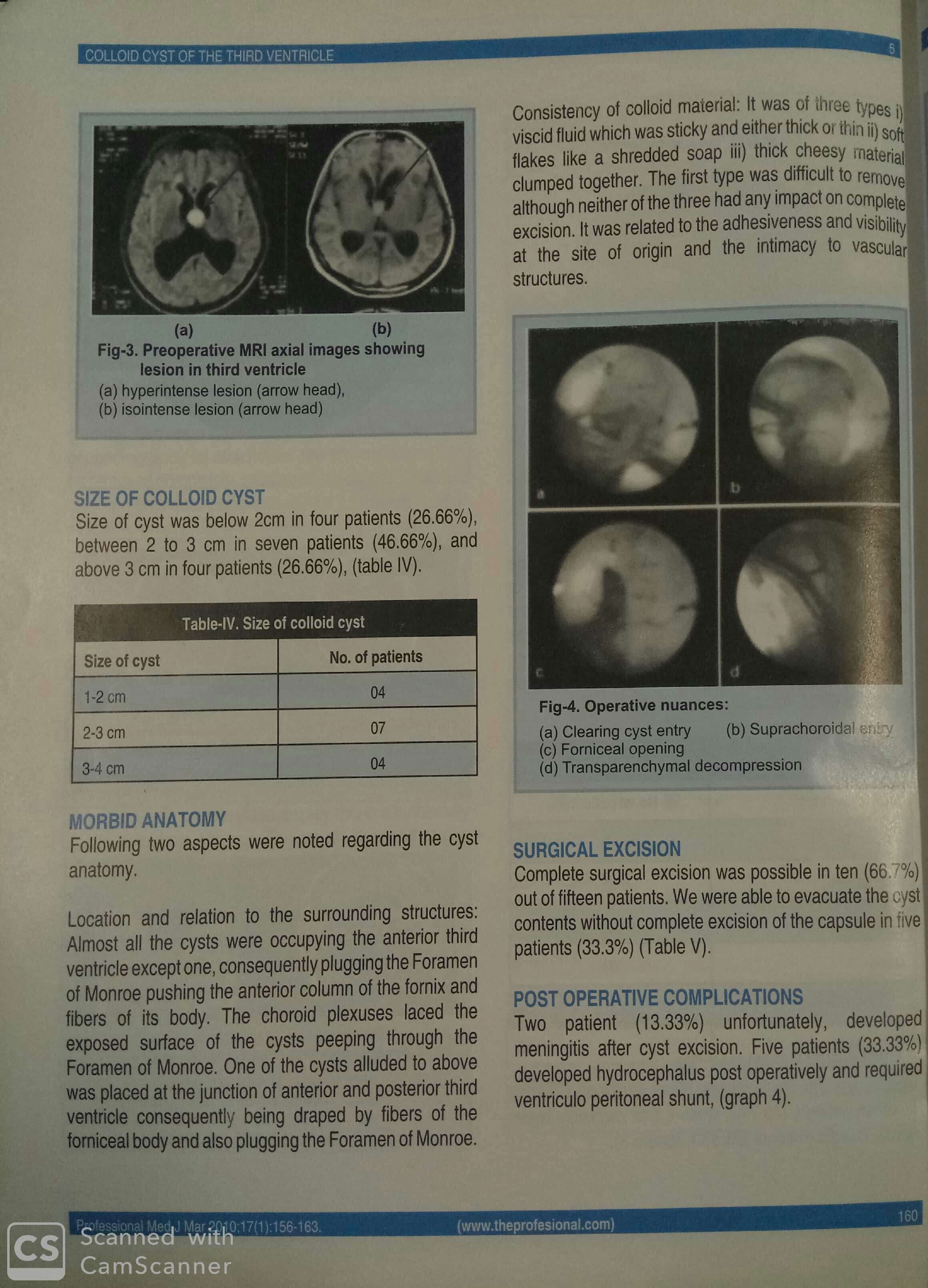
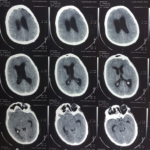
- T1 without Contrast MRI
-
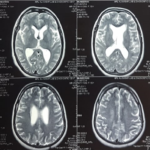
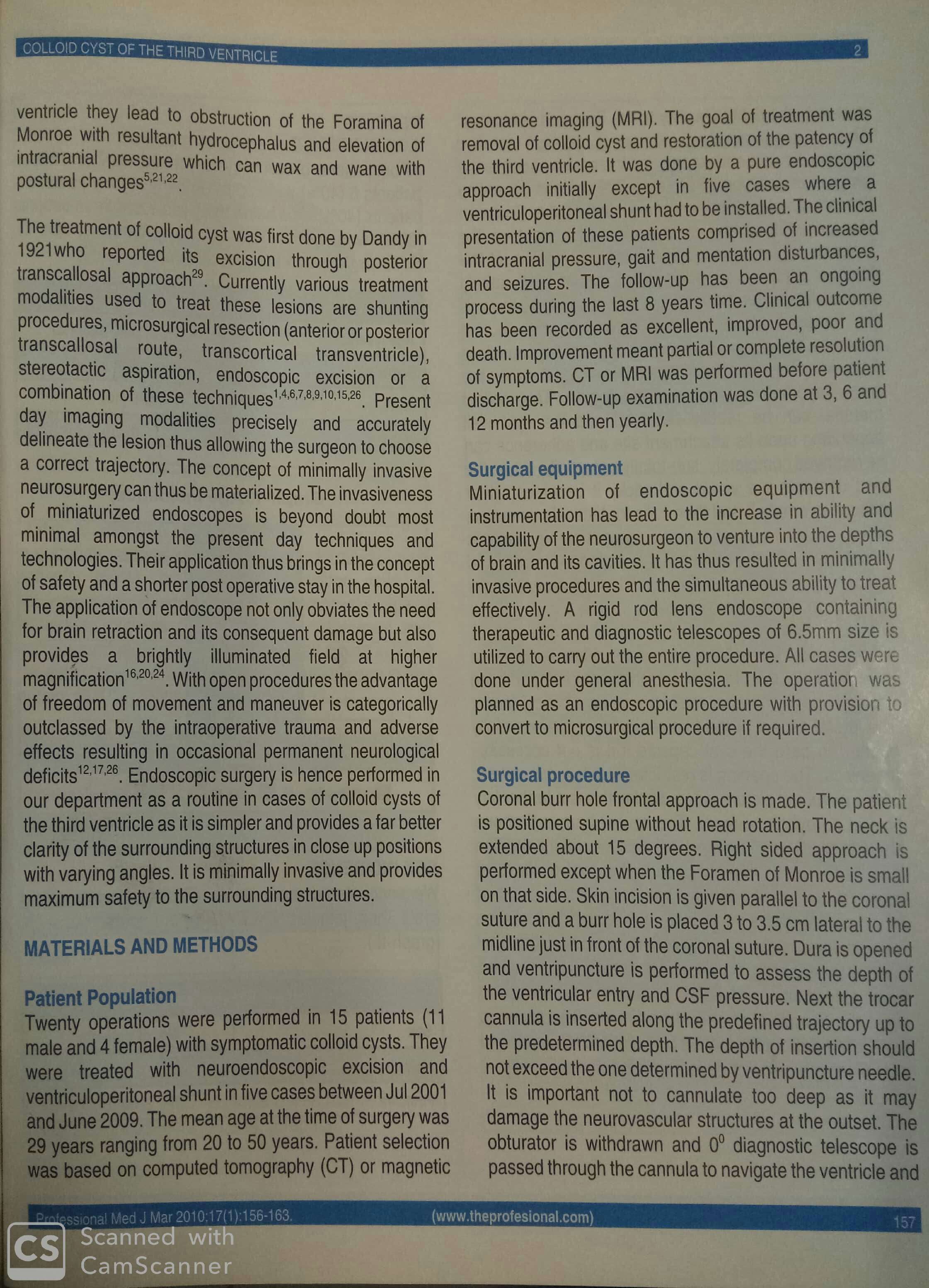
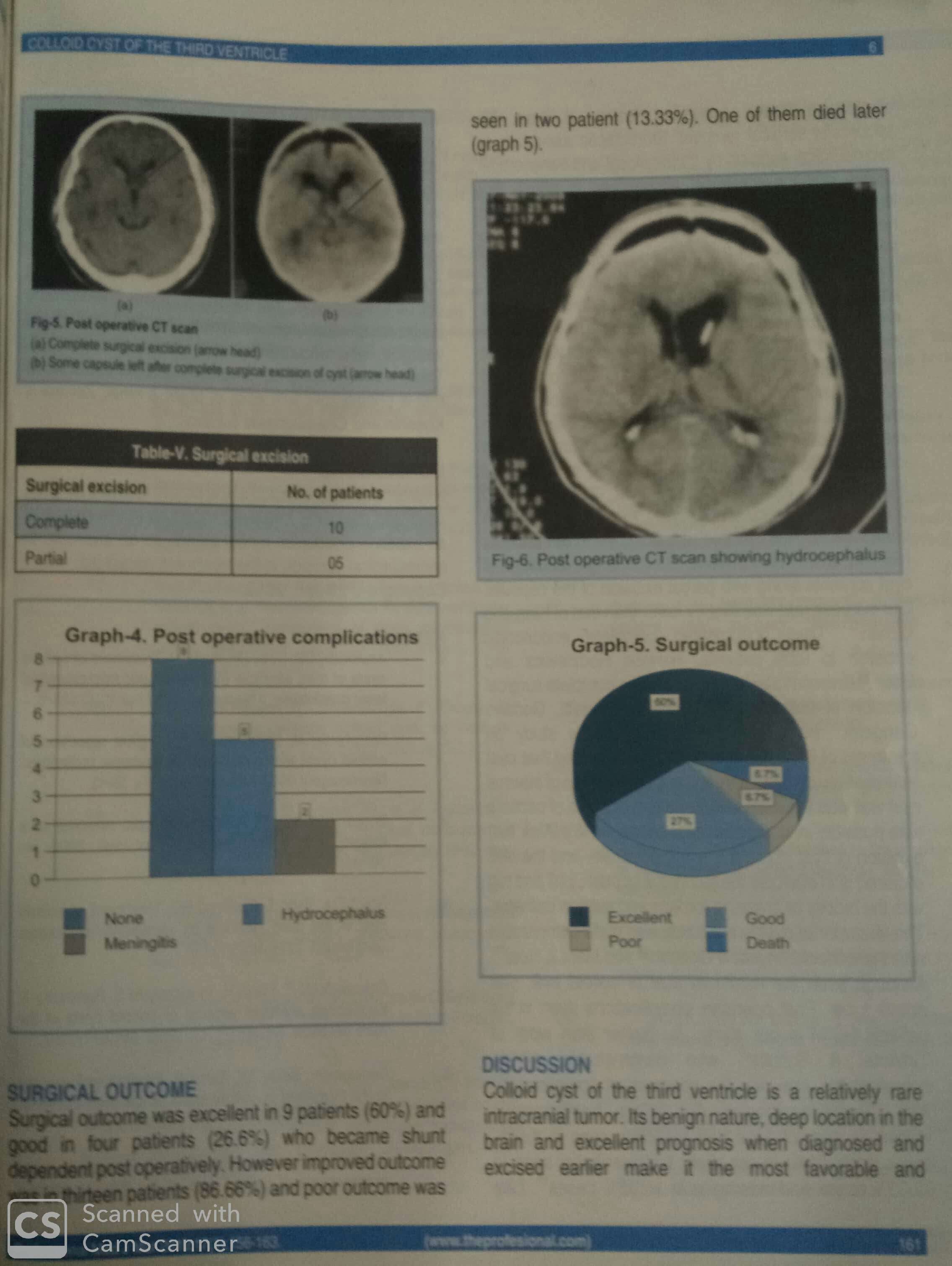
- T2 Weighted MRI
-
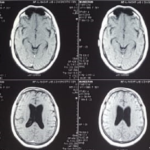
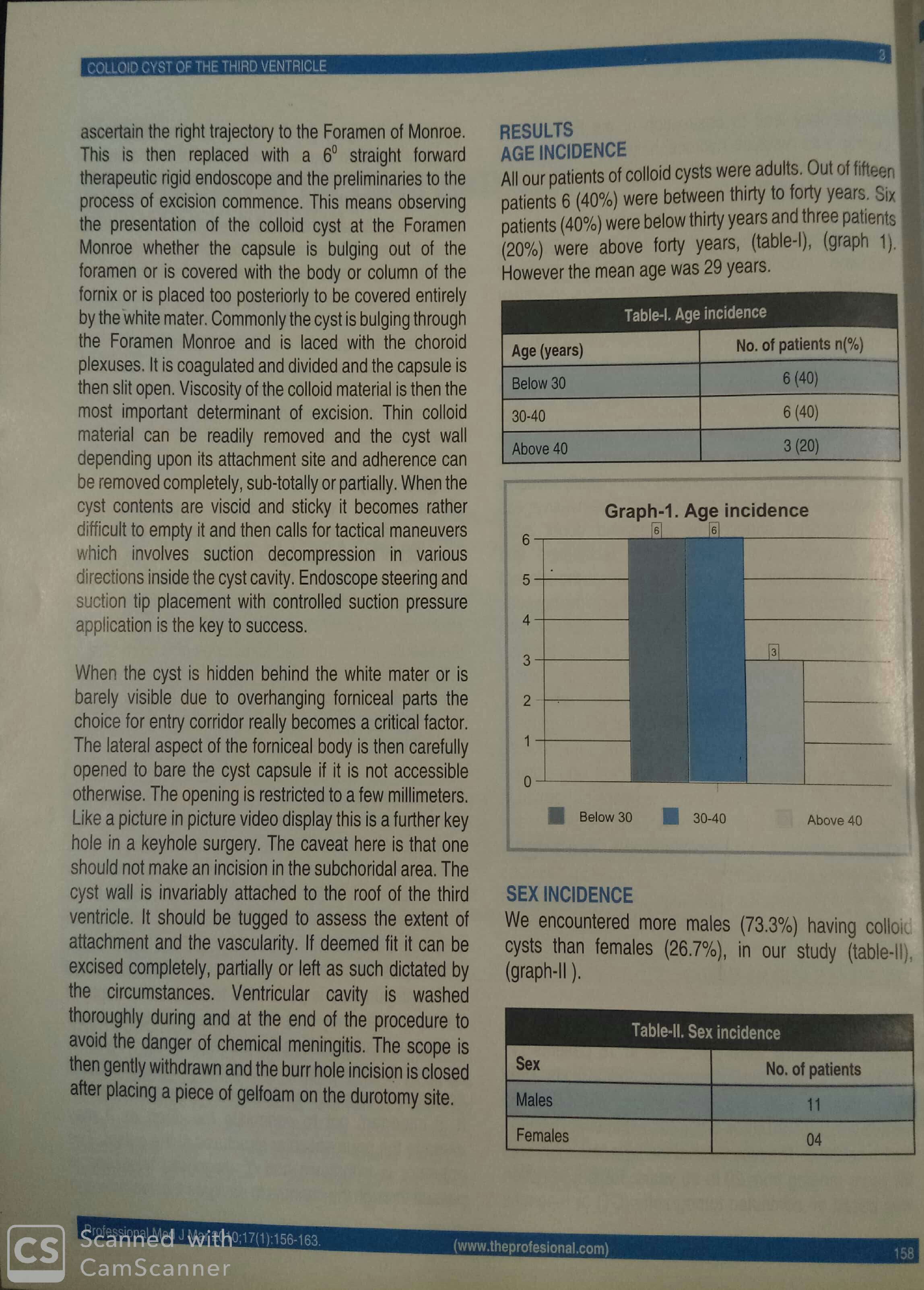
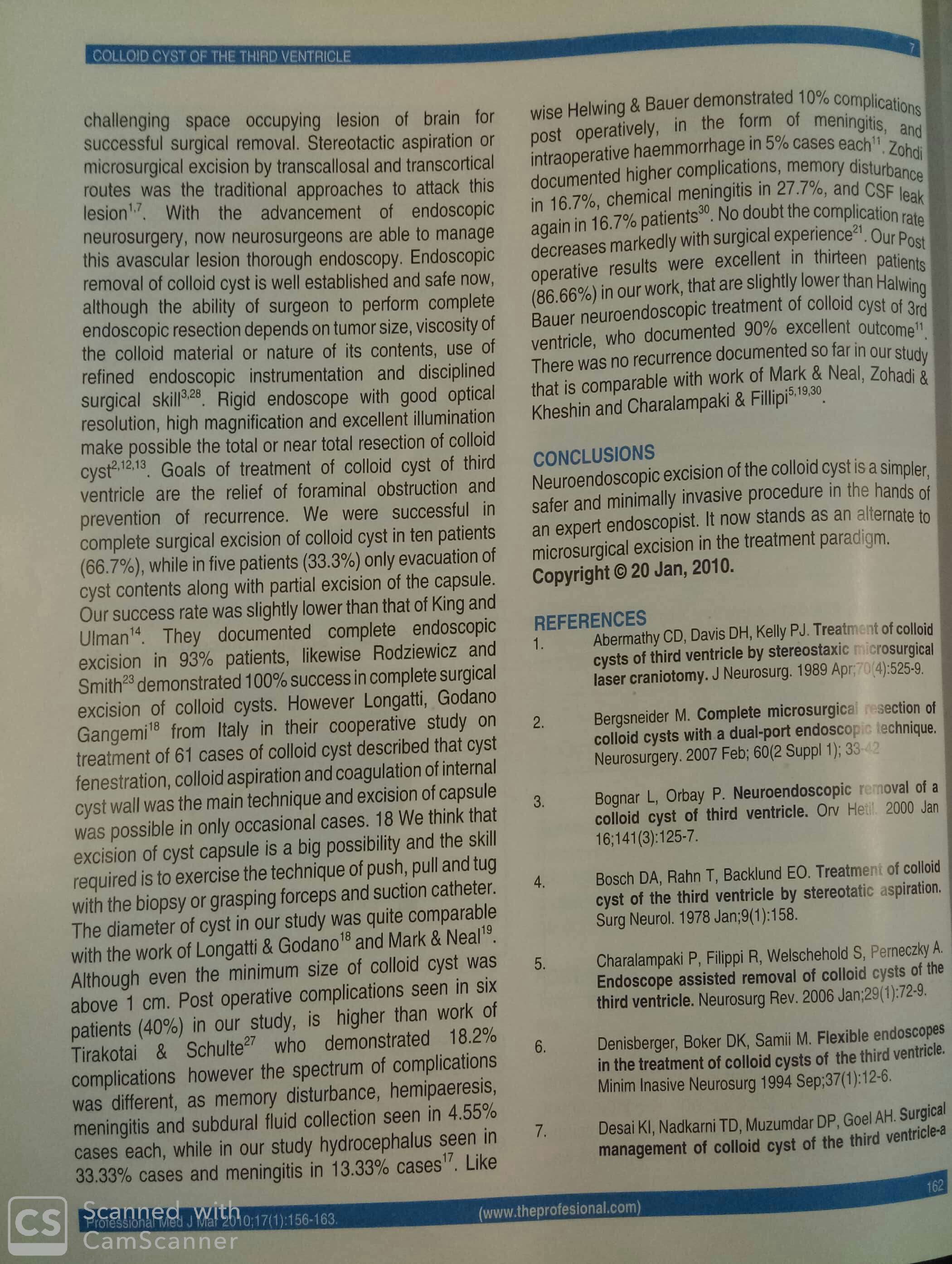
- T1 With Contrast MRI
-
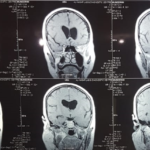
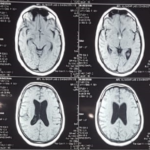
- Coronol MRI
-
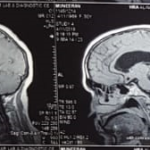
- Sagittal MRI
Jinnah Hospital, Usmani Road,
Lahore, Pakistan
A middle aged lady presented to emergency department with sudden headache and altered conscious level. On Examination she had GCS 10/15. No focal neurological sign. Papilledema was present. CT Scan Brain showed hyperdense third ventricular Colloid cyst with Hydrocephalus.
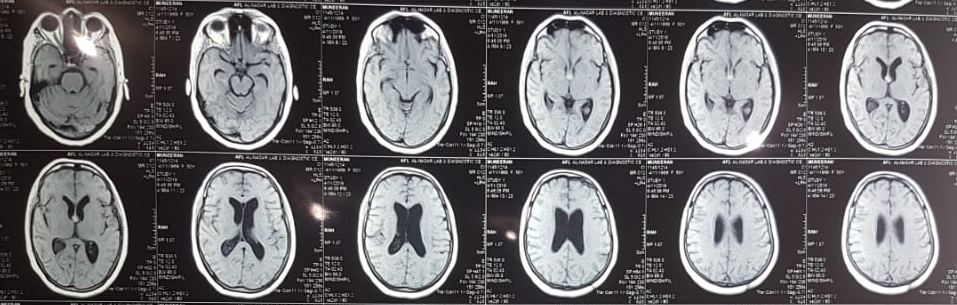
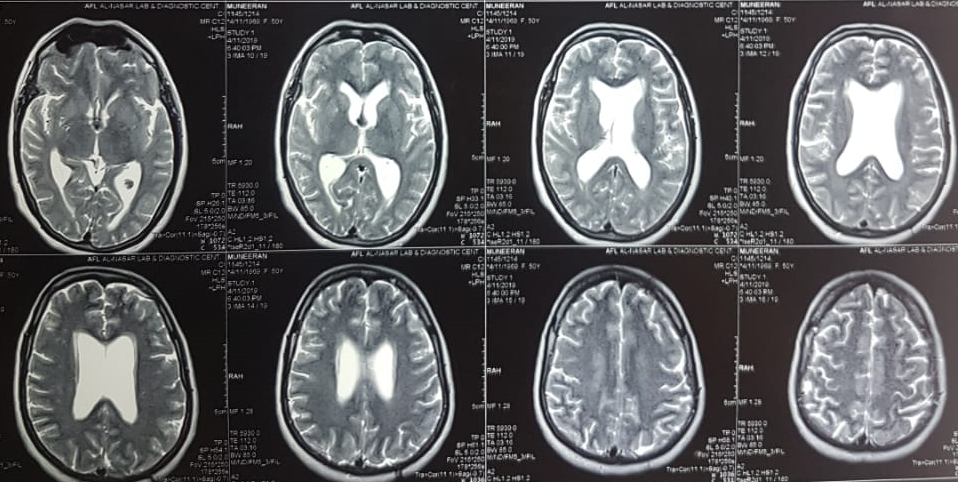
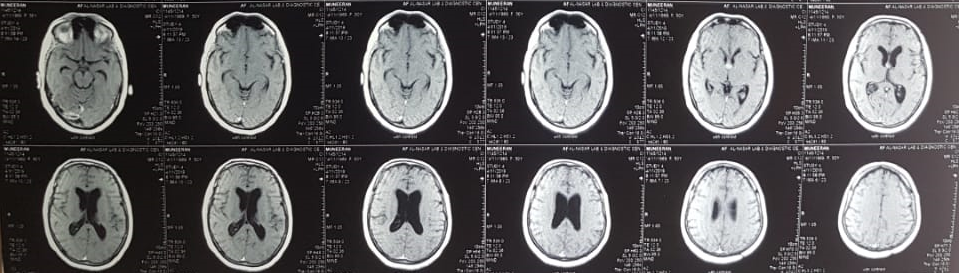
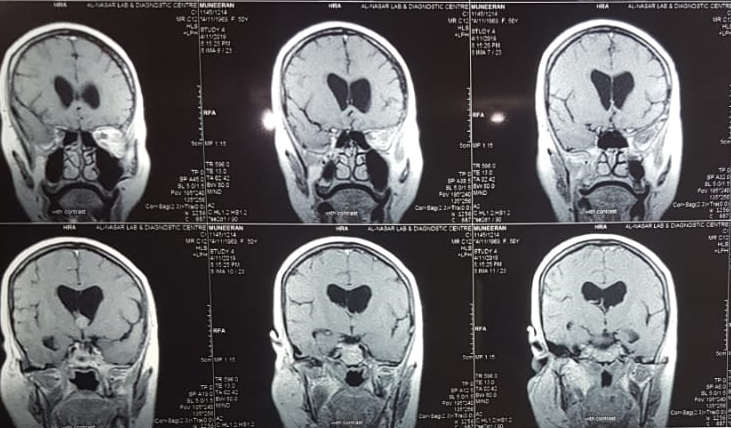

MRI Brain showed hyperintense cyst on T1 images and hypointense on T2 weighted image: high proteineous contents and less fluidy. These features are consistent with firm to hard consistency of cyst.
Endoscopic excision of colloid cyst was planned.
Colloid cysts of the third ventricle are benign epithelial lined cysts, usually asymptomatic, they can rarely present with acute and profound hydrocephalus.
Colloid cyst is uncommon entity and account for ~2% (range 0.5-3%) of primary brain tumors and 15-20% of intraventricular masses . They are located at the foramen of Monro in 99% of cases.
The majority of cases are identified in early middle age (30-40 years of age), rarely in pediatrics age group.
Colloid cysts originate from the abnormal folding of the primitive neuro-epithelium (the paraphysis elements).
These cysts are lined by a single layer of columnar epithelium which produces mucin, which appears as a thick yellow-green fluid when the cyst is open.
Radiological features are highly variable depending upon composition of cyst. T2 signal intensity of the cyst (low signal = difficult to aspirate). FLAIR: cysts which are of low signal on T2 will appear similar to attenuated CSF on FLAIR, and are thus difficult to appreciate.
Reference: Radiopedia