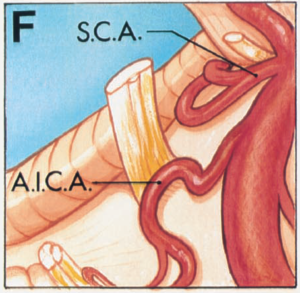
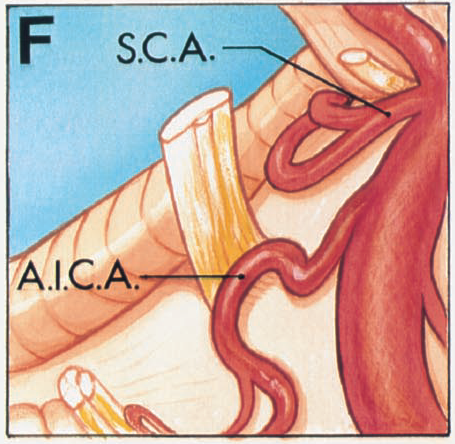
In 1934, Dandy postulated that arterial compression and distortion of the trigeminal nerve might be the cause of trigeminal neuralgia. He described the superior cerebellar artery (SCA) as affecting the nerve in 30.7% of his 215 cases of trigeminal neuralgia. The vascular compression theory failed to gain acceptance at the time, but it awaited the better demonstration of these pathological changes at surgery by Jannetta using magnification provided by the operating microscope.
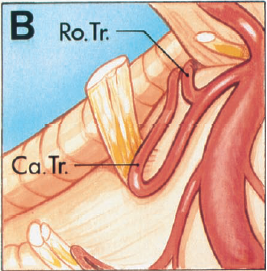
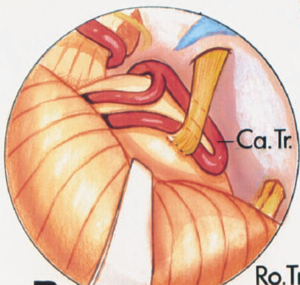
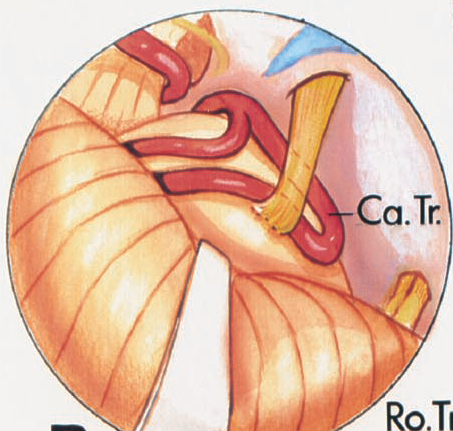
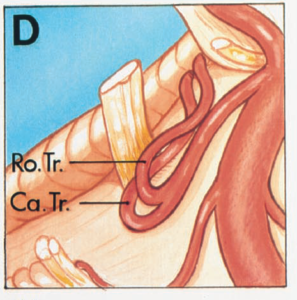
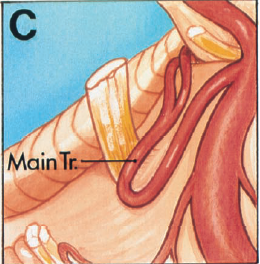
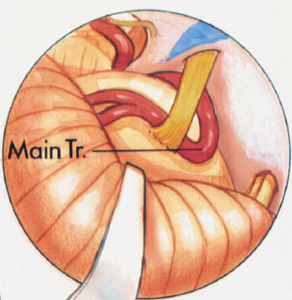
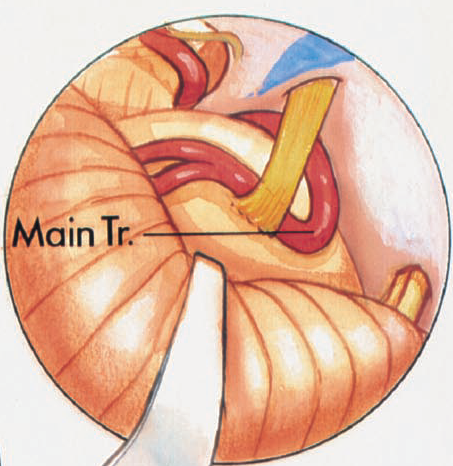
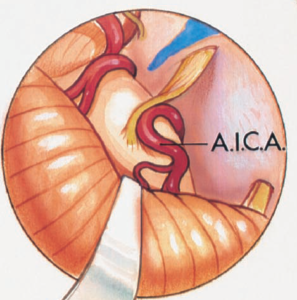
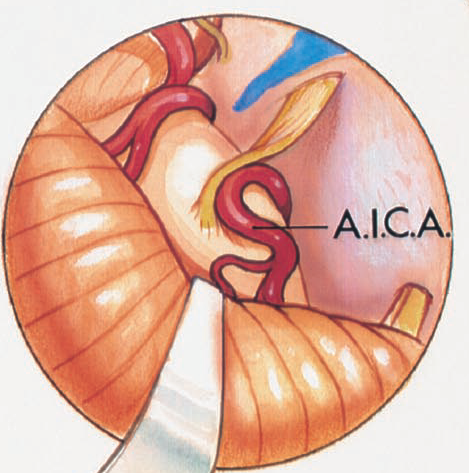
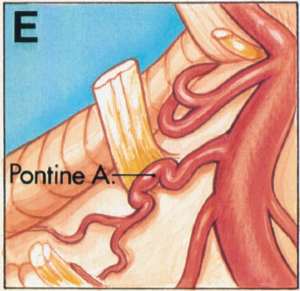
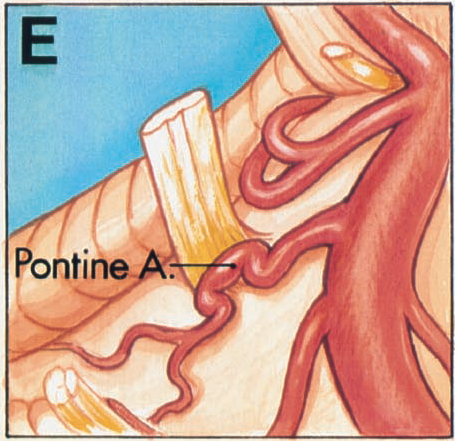
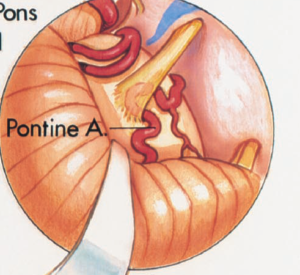
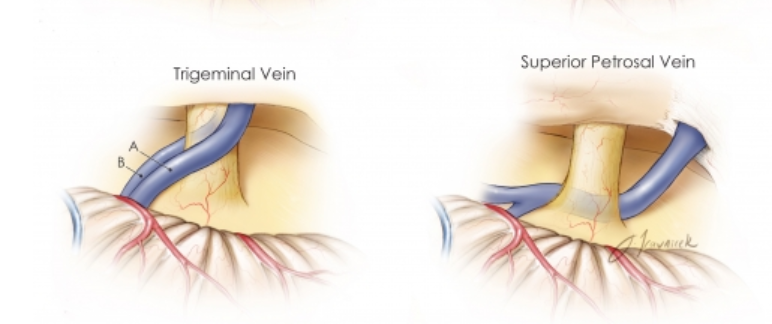
However, other sites of compression are seen, depending on how far distal the artery bifurcates in relation to the trigeminal nerve.
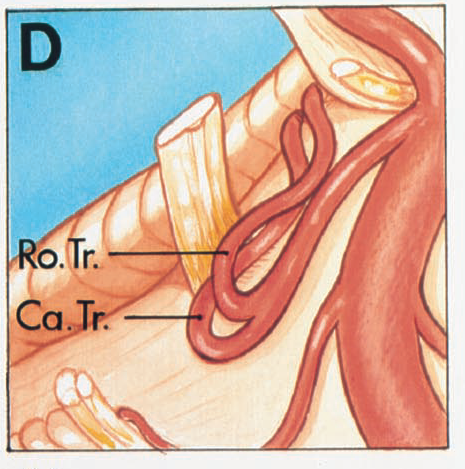
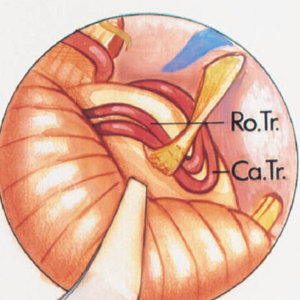
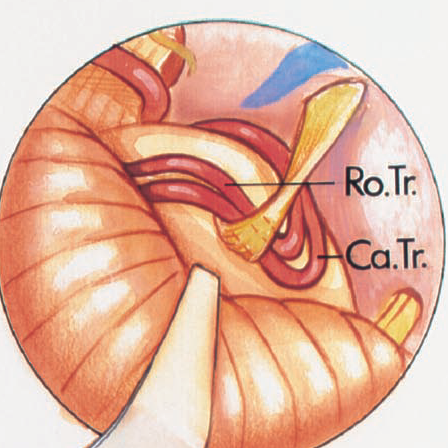
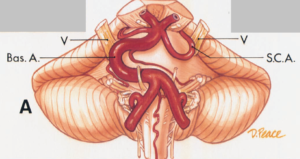
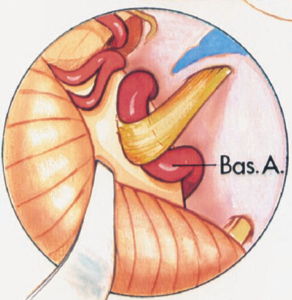
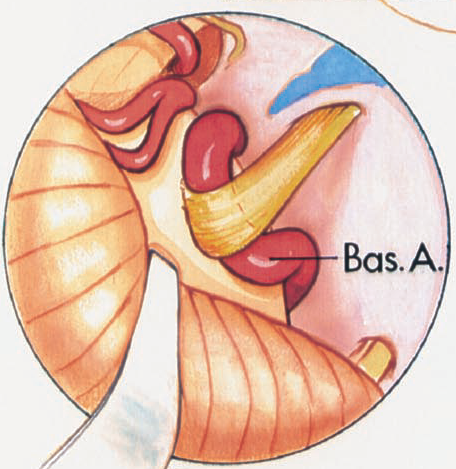
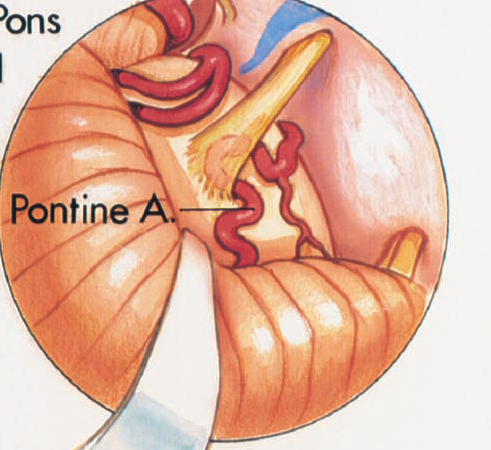
If the SCA bifurcates near the basilar artery or if there is a duplicate configuration in which the rostral and caudal trunks arise directly from the basilar artery, both trunks may loop down into the axilla and compress the nerve.