Intracranial Pressure Monitoring: Important Tool in Severe Head Injury Management
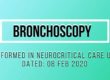
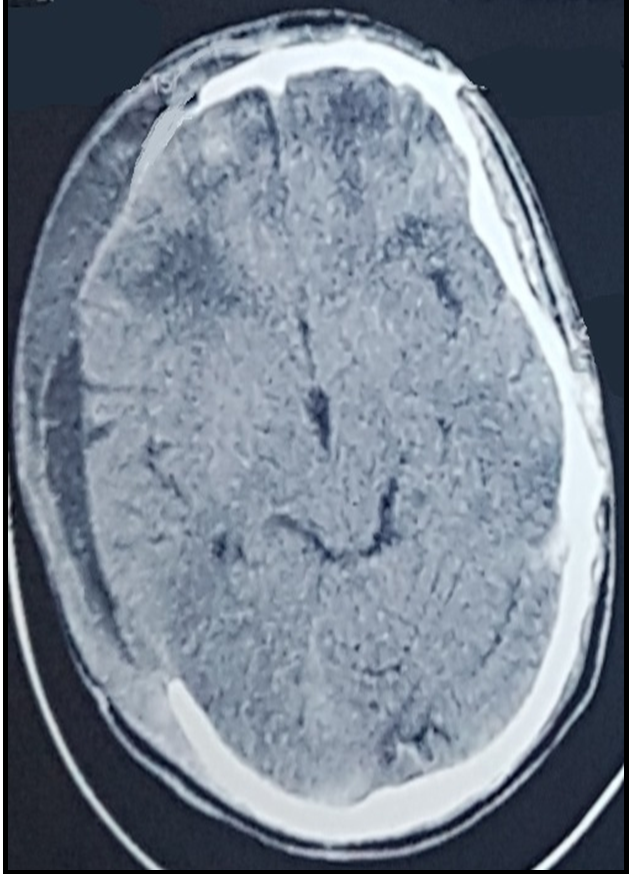
A young 30 years male was presented with road traffic accident with GCS 6/15. Initial CT Scan showed small frontal contusion with basal cisternal obliteration. So ICP cather was placed and patient was managed conservatively in ICU.
Gradually ICP readings began to rise and became non responsive to osmotic therapy.
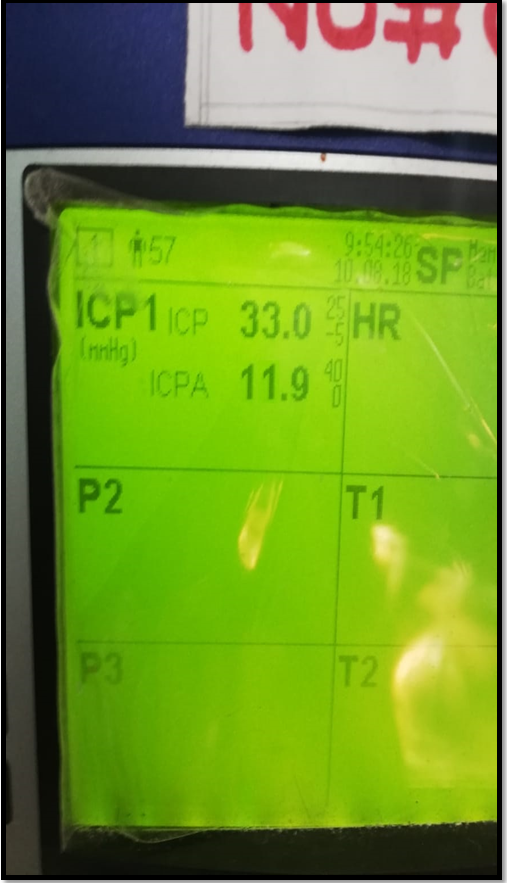
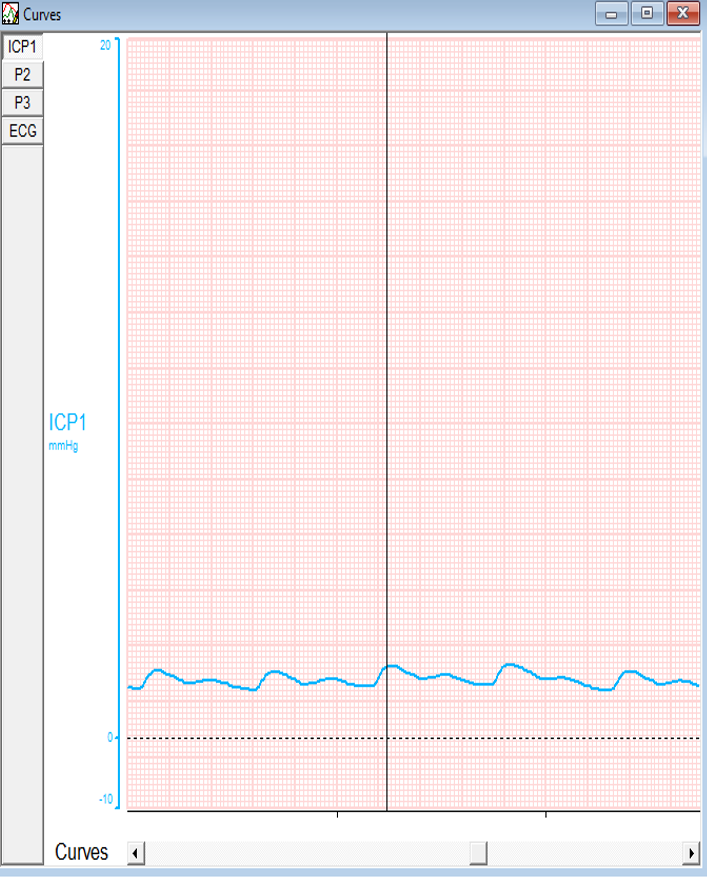
Repeat CT showed enlargement of frontal contusion. ICP was approaching to 37 and ICP A is 14 that is reflected the abnormal waveform.
As per our protocol ICP surge greater than 25mmHg, resistant to conservative therapy, decompressive craniotomy was planned.
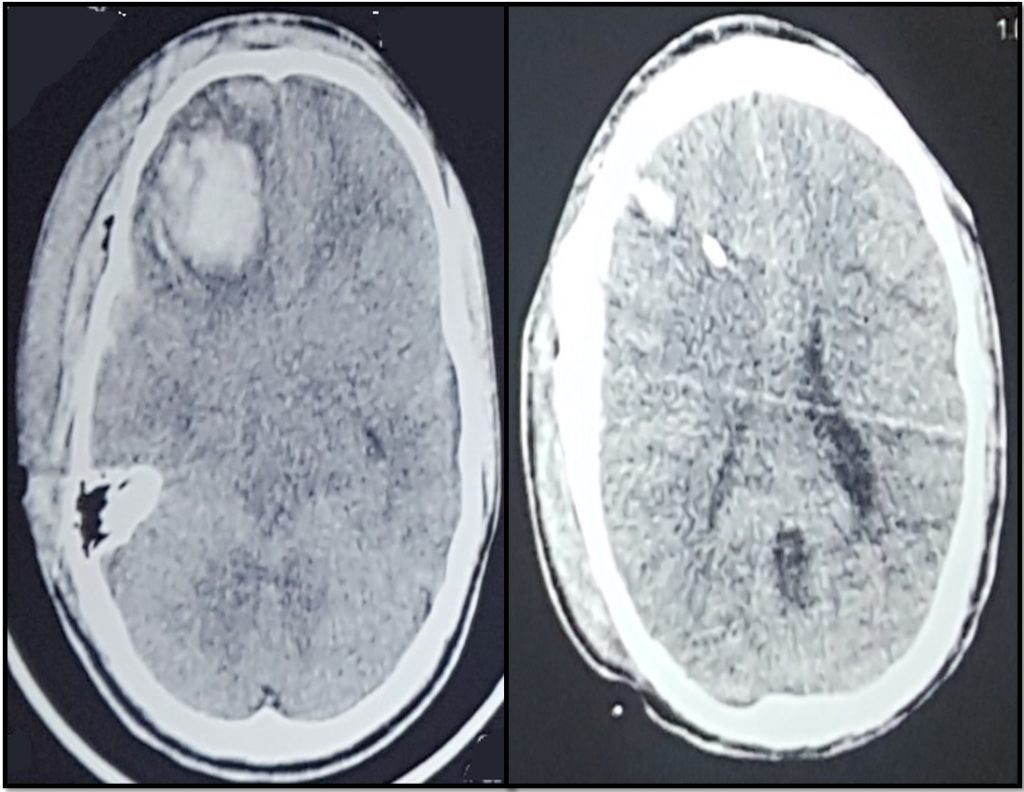

Pre Operative Readings
P2 is taller than P1: Poor Compliance
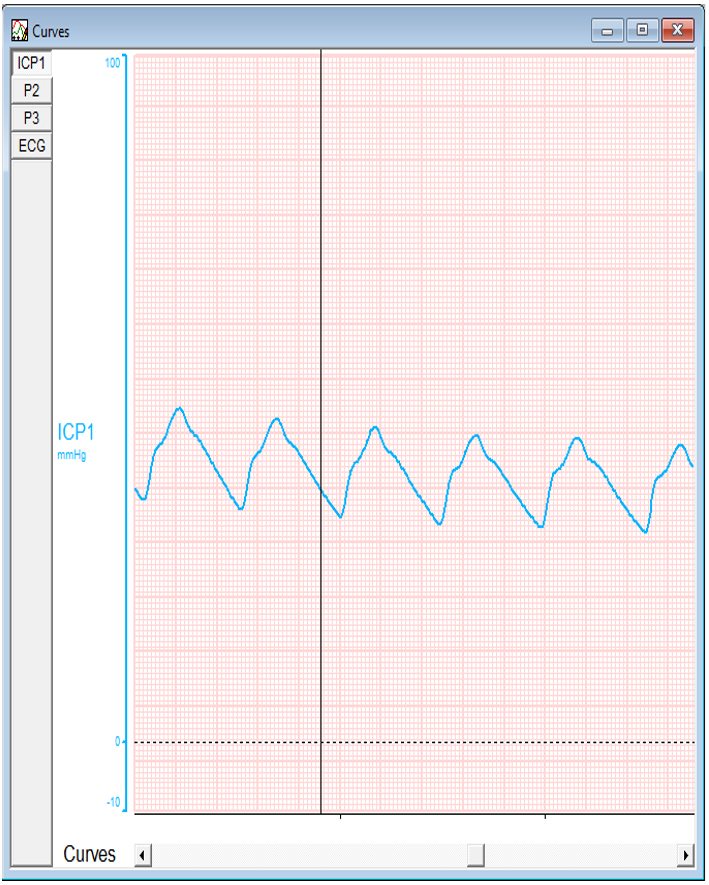
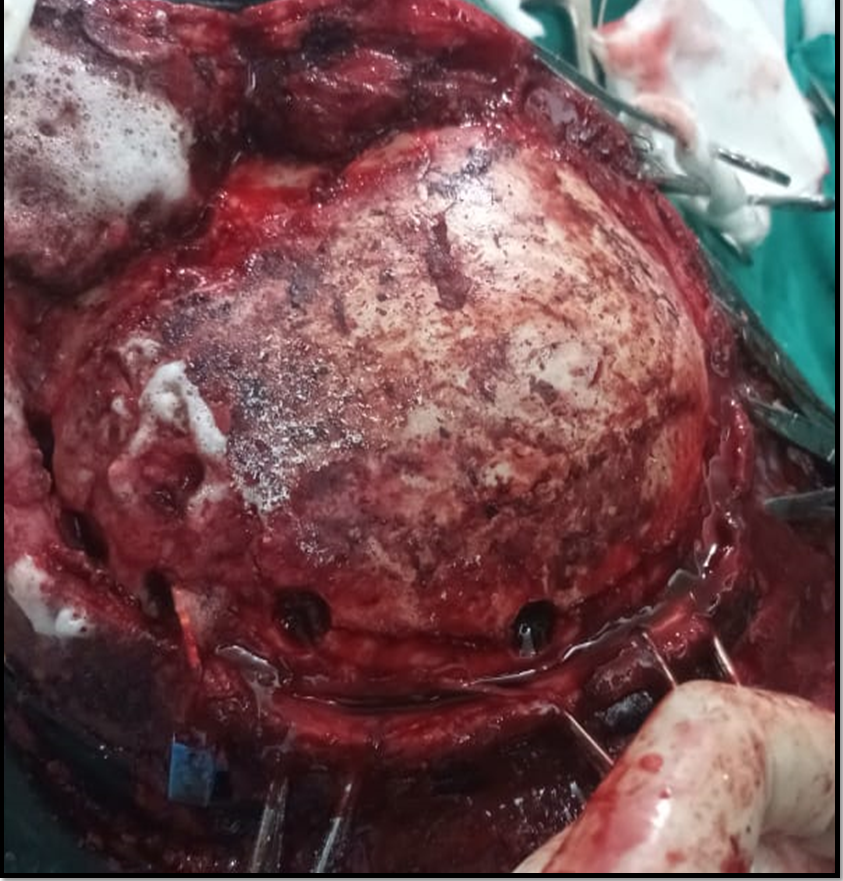
Upon lifting the bone flap there is a minimal drop in both values but still in high range.
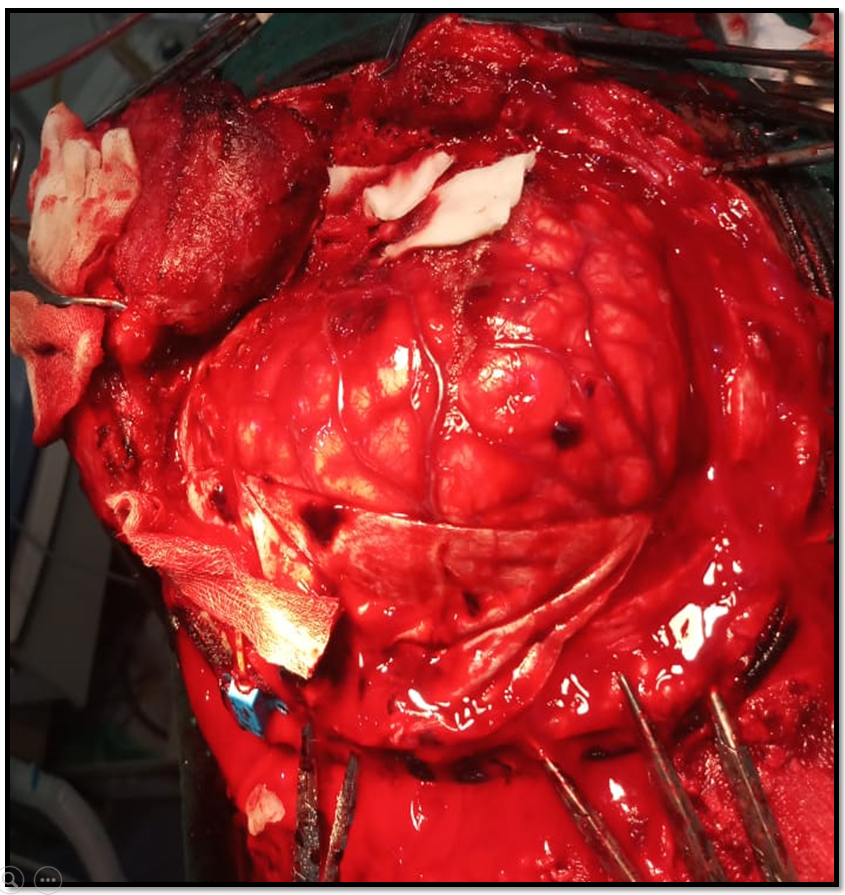
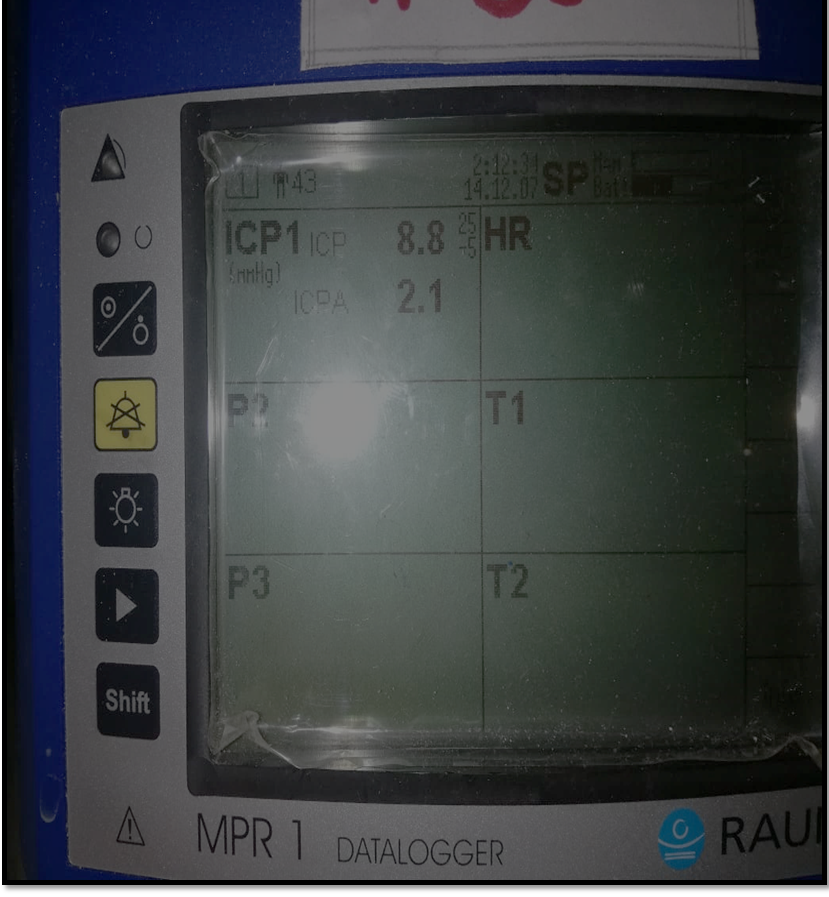
As durotomy is done, both ICP and ICP A again plummet to the normal values, also evidenced by the graph.
Post op ct scan showing adequate decompression.
Discussion
The volume of the skull contains approximately 85% brain tissue and extracellular fluid, 10% blood, and 5% CSF. If brain volume increases, for example contusion in head injury, there is a compensatory displacement of CSF into the thecal sac of the spine followed by a reduction in intracranial blood volume by vasoconstriction and extracranial drainage. If these mechanisms are successful, ICP remains unchanged. Once these mechanisms are exhausted, further changes in intracranial volume can lead to dramatic increases in ICP.
Elevated intracranial pressure (ICP) is seen in many pathological brain conditions including head trauma. Intractable elevated ICP can lead to death or devastating neurological damage either by reducing cerebral perfusion pressure (CPP) and causing cerebral ischemia or by compressing and causing herniation of the brainstem or other vital structures. Elevated ICP needs prompt recognition for treatment measures. A mechanical ventilated patient of severe traumatic brain injury has limited clinical signs to show for identification of elevated ICP or clinically recognition of efficacy of treatment on ICP. Continuous ICP monitoring is important both for assessing the efficacy of therapeutic measures and for evaluating the evolution of brain injury.
The goal of ICP monitoring is to ensure maintenance of optimal Cerebral Perfusion Pressure(CPP). The ICP also forms a basis for medical or surgical intervention in cases of increased ICP with agents such as 3% sodium chloride (NaCl), mannitol, or diuretics (Lasix), ventriculostomy, cerebrospinal fluid (CSF) diversion, and pentobarbital coma or surgical decompression in cases of intractable ICP elevation that do not respond to conservative management.
Reference:
https://emedicine.medscape.com/article/1829950-overview