Intramedullary Mature Teratoma of the Conus Medullaris
A 60 years male was presented in outpatient department with right leg weakness since childhood, and progressive weakness of left leg, pain left leg and sphincteric involvement since two months. Previously he was able to walk with minimal disability, since the weakness of left leg progressed he was unable to walk without walker support. He had history of right two little toe amputations due to non healing ulcer 10 years ago.



His examination showed decreased bulk on right side, power 2/5 on right side, and 4/5 on left side. Absent knee and ankle jerks on right side. Diminished left knee and absent ankle reflex. Back has tuft of hair on back.

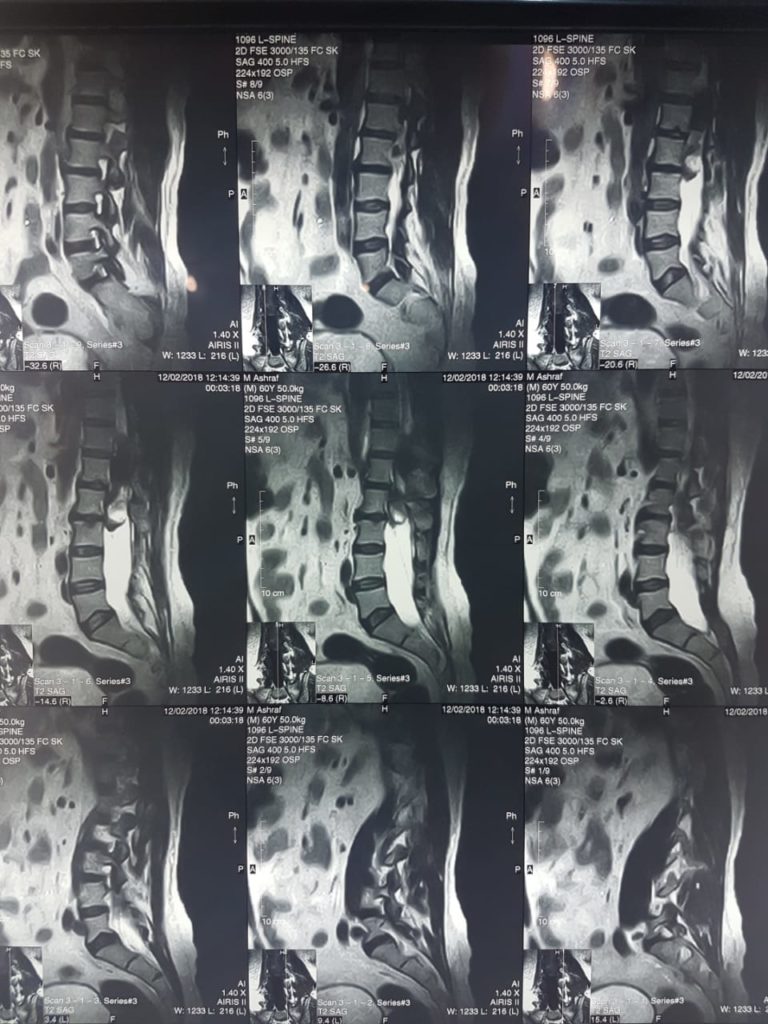
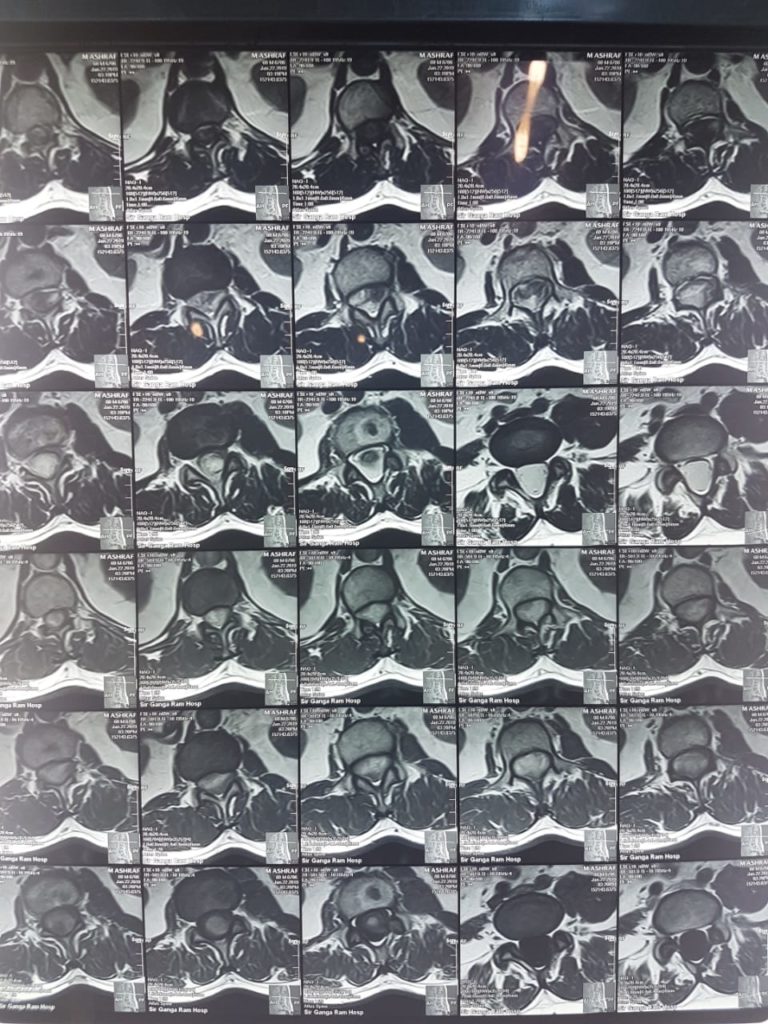
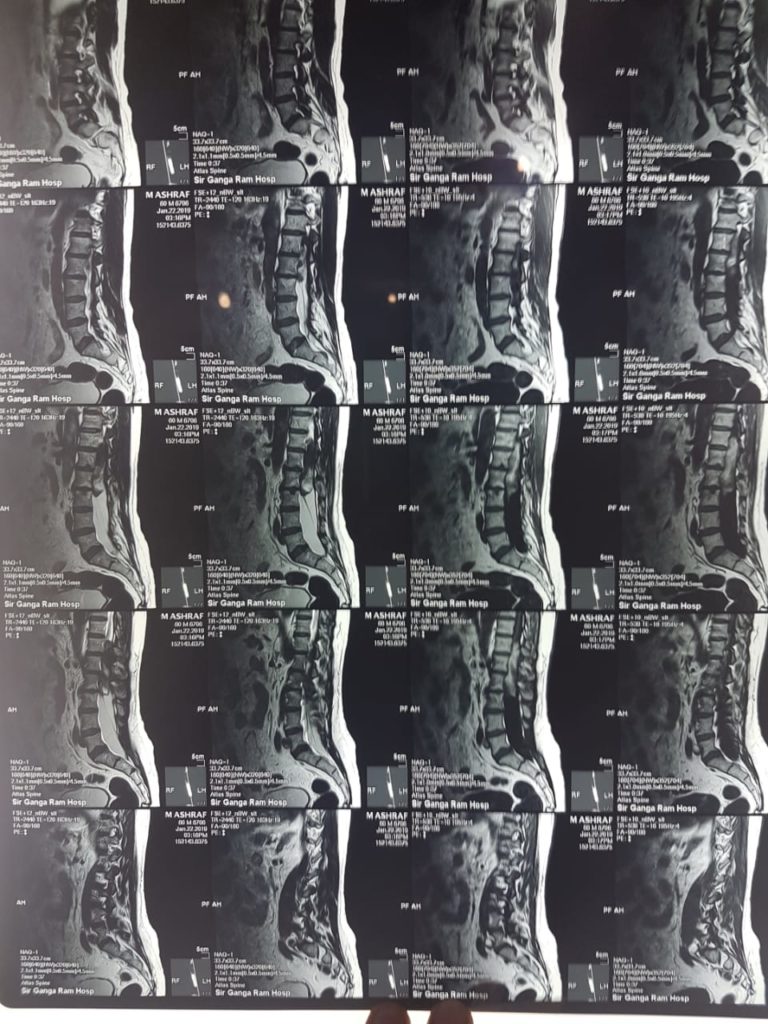
Bifid spine of L4 and 5 Lumbar vertebrae. MRI showed D12 to L3 non enhancing intramedullary SOL.
To our surprise histopathology showed Mature Teratoma.
Discussion
Teratomas are a type of multipotential cell tumor that contain a mixture of multiple germinal layers formed by normal organogenesis and reproductive tissues.
The incidence of spinal teratoma is rare; only 0.15–0.18% of spinal tumors have been classified as teratomas. In pediatric patients, ~5–10% of spinal tumors are intraspinal teratomas, however, the incidence in adult patients is significantly lower than that observed in children and infants.
The tumors are predominantly located between the lower thoracic vertebrae and the conus medullaris level.
The morphological presentation varied in the MRI scans according to the location of the tumors. Intradural teratomas are commonly oval or lobulated heterogenous masses, whereas extradural teratomas were more commonly observed to be dumbbell-shaped. Cases of extradural teratoma are commonly accompanied with vertebral body misformation, while adult intradural teratomas are typically located beneath the dura, rarely invading the dura or vertebral body.
There are two dominant theories regarding the origin of intraspinal teratomas. The first is the dysembryogenic theory, and the second is the misplaced germ cell theory.
The dysembryogenic theory indicates that spinal teratomas arise from pluripotent cells, and that in a locally disturbed developmental environment, these pluripotent cells differentiate chaotically. When such disordered development occurs in a primitive streak or a caudal cell mass, a spinal teratoma forms. The misplaced germ cell theory suggests that certain pluripotent primodial germ cells of the neural tube are misplaced during migration from the yolk sac to the gonad, thus resulting in spinal teratoma formation.
Literatute review shows that till now only less than 25 cases of adult intradural teratoma are reported.
Mature intradural teratomas in adults are rare, with few accompanying spinal anomalies. The currently preferred theory of origin of the disease is the misplaced germ cell theory. A resection of the tumor is the primary treatment methodology for adult patients, as the nature of the tumor is relatively benign and the recurrence ratio is low, even following gross resection. However, radiosurgery is not recommended.
Reference:
Li Y, Yang B, Song L, Yan D. Mature teratoma of the spinal cord in adults: An unusual case. Oncol Lett. 2013;6(4):942-946.